Racing to Stop a Pandemic: The Critical Role of Clinical Trials
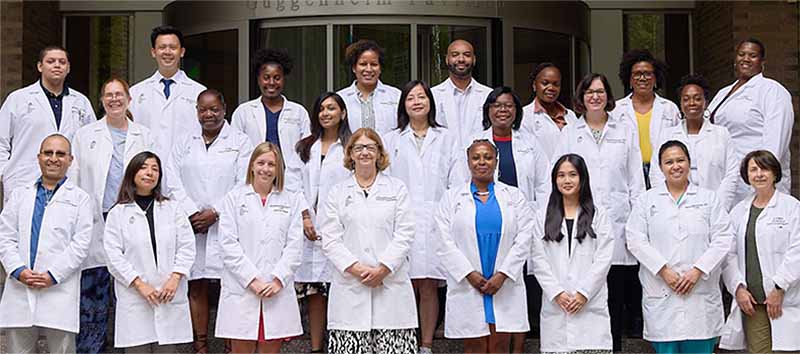
A group photo of the COVID-19 Clinical Trial Unit, part of the Mount Sinai Infectious Diseases Clinical and Translational Research Center.
When the COVID-19 pandemic ramped up in New York City in March 2020, the disease was so novel there was no approved treatment for it.
“We saw people come to the hospital with COVID-19, and without specialized treatments, many died,” said Sean Liu, MD, PhD, Associate Professor of Medicine (Infectious Diseases) at the Icahn School of Medicine at Mount Sinai. “I remember feeling helpless, and helplessness is probably the worst feeling that a doctor could experience, because people come to you for help but there is only so much you can do or give.”
With a dire need to discover treatments for patients, the Mount Sinai Infectious Diseases Clinical and Translational Research Center (CTRC) formed the COVID-19 Clinical Trial Unit (COVID CTU) in June 2020 to find ways to stop the disease.
“We already had experts beginning the effort, and with the support of Dennis S. Charney, MD, Anne and Joel Ehrenkranz Dean of the Icahn School of Medicine, and under the leadership of Judith Aberg, MD, Director of the CTRC, we were able to form the COVID CTU and go all in to stop COVID-19,” said Dr. Liu, who was tapped as Medical Director of the research unit.
The COVID CTU conducted interventional studies in all aspects of tackling COVID-19, including several drugs that were ultimately approved by the U.S. Food and Drug Administration (FDA). These include Regeneron’s monoclonal antibody therapies, Gilead Sciences’ remdesivir, and two COVID-19 vaccines.
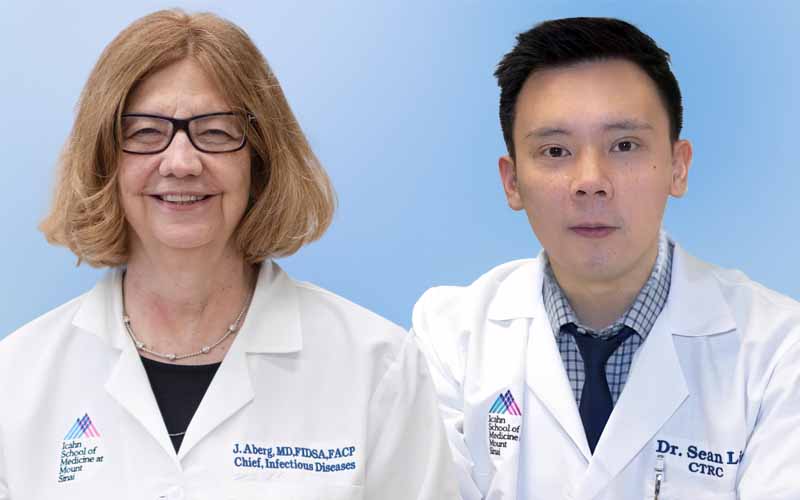
Judith Aberg, MD, Director of the Mount Sinai Infectious Diseases Clinical and Translational Research Center (left) and Sean Liu, MD, PhD, Medical Director of the COVID-19 Clinical Trials Unit (right).
In this Q&A, Dr. Liu and Dr. Aberg share their experience of how the COVID CTU worked tirelessly throughout the pandemic, and where it is headed in the future.
How did the COVID CTU come to be formed?
Dr. Aberg: We were able to build upon the infrastructure that was created for HIV clinical trials, along with the support of many, to immediately start two different drug trials for COVID-19. One drug aimed at the SARS-CoV-2 virus and the other was a potent anti-inflammatory. And I must say, our prompt efforts paid off. We were able to give remdesivir, an antiviral drug, via a compassionate use application on March 9—within two days of the admission of our first patient at Mount Sinai West.
Dr. Liu: When the pandemic first hit, I was working as a hospitalist—someone who cares for admitted patients—at Mount Sinai Queens, and Dr. Aberg asked me to help with clinical trials at The Mount Sinai Hospital.
As pharmaceutical companies started developing more candidates for COVID-19 treatment, the team working on the initial studies started taking on more studies, supported by the CTRC, the Infectious Diseases Division, and the Medicine Clinical Trials Office at the Icahn School of Medicine. When we realized we sorely needed to expand and formalize a team for COVID-19-related trials, Dean Charney provided seed funding, and during the summer of 2020, we were able to hire more staff needed to run the trials.
How big was the COVID CTU then, and how has it grown since?
Dr. Liu: It started with 11 people, including six from the CTRC. By 2021, we had 25 staff.
What was it like fielding a clinical trials team during the pandemic?
Dr. Liu: Dr. Aberg already had a research unit working with HIV before the pandemic, and we pooled together a staff of clinical researchers, project managers, research nurses, coordinators, and regulatory staff. It was incredible seeing so many people come together quickly to tackle one of the biggest challenges we’ve faced in health care.
In addition to assessing the effectiveness of industry-developed treatments, the unit became a translational springboard where basic science researchers could come to us with their ideas, and we could help apply them in a phase 1 study, creating a bridge between preclinical and in-human studies.
What were some of the COVID-19 trials done at Mount Sinai?
Drs. Aberg and Liu recall some of the studies done by the COVID CTU:
- Remdesivir: The antiviral drug is currently approved by the FDA to treat patients hospitalized for COVID-19. We initially opened trials for this drug via an emergency investigational new drug application at seven hospitals. In less than a month, we opened the Gilead-sponsored studies at four hospitals.
- Monoclonal antibodies (mAbs): We were involved in Regeneron’s mAb studies in many different settings. These included an outpatient treatment study, an outpatient post-exposure prophylaxis study, and a pre-exposure prophylaxis study. One of Regeneron’s mAb that we did a study on was sarilumab, a potent IL-6 inhibitor. While this study did not demonstrate the robust findings of another IL-6 inhibitor we had worked on, Roche’s tocilizumab, it was the first study that paved the way for potent immune-modulating therapies to treat COVID-19 as we do currently.
- mRNA vaccine: We were heavily engaged in the Pfizer/BioNTech COVID-19 vaccine trial, enrolling hundreds of participants from diverse backgrounds. Mount Sinai was recognized for enrolling the 40,000th participant in the initial phase 3 trial.
- NDV-HXP-S: Mount Sinai developed its own COVID-19 vaccine, which can be delivered via injection or the nose. The technology was developed by our Microbiology Department, and the COVID CTU helped run the phase 1 trial. With our data, the vaccine went on to be developed further in other countries and has gone on to be approved as booster shots in Mexico and Thailand.
- Hyperimmune immunoglobulin: This was a blood product-derived treatment using extracted antibodies from a pool of convalescent plasma donors who had recovered from COVID-19. With hyperimmune immunoglobulin, the patient is receiving a known purified amount of antibody from the donor. Studies are ongoing to identify who would benefit the most as well as timing in relation to onset of symptoms.
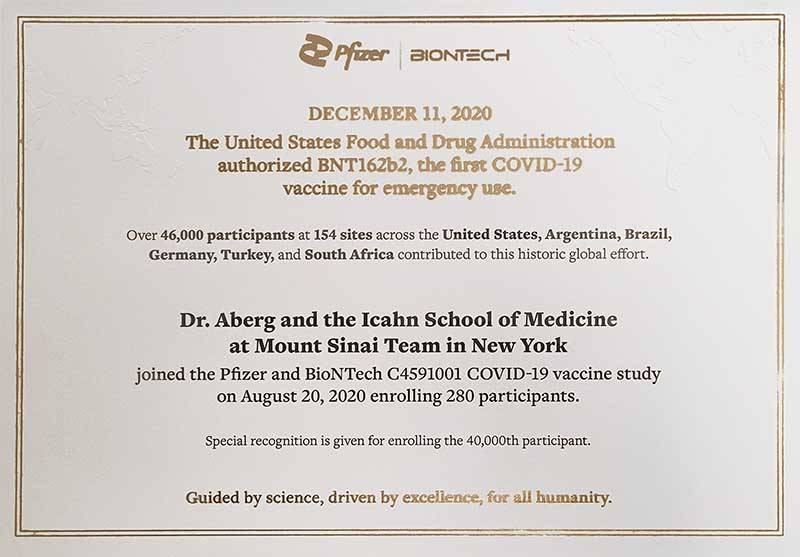
The COVID Clinical Trials Unit team received a letter of recognition for enrolling 280 participants—as well as the 40,000th participant—in the Pfizer/BioNTech COVID-19 vaccine trial.
What were some lessons learned on running clinical trials to address the pandemic?
Dr. Liu: There were so many studies to undertake, but we had to learn to focus. A part of it was trial and error, but as we gained experience, we became better at identifying what studies were likely to yield promising results. Some clinical trials might sound great on paper, but given limited resources, we had to weigh what factors went into them—such as enrollment opportunity or viral targets—and choose our trials accordingly or make adjustments.
Dr. Aberg: Decisive action can help change the trajectory of a pandemic. When Regeneron finalized its protocol for sarilumab trials, within seven days we opened a randomized, placebo-controlled trial of the drug. Its interim results, along with our remdesivir clinical trials and observational use of tocilizumab, helped advise us of the narrow window where these types of drugs may be effective to prevent patients from developing respiratory failure, requiring them to go on a ventilator, and even death.
What’s next for the COVID CTU?
Dr. Aberg: The COVID CTU no longer needed to be distinct from the CTRC. However, we are still involved in COVID-19 studies. One such trial is RECOVER-VITAL, a National Institutes of Health (NIH)-funded study to explore whether Pfizer’s Paxlovid™ treatment can be used to treat the chronic disease state commonly referred to as long COVID.
We are also in the NIH-funded Strategies and Treatments for Respiratory Infections and Viral Emergencies (STRIVE) consortium. A COVID-19 study we are involved in as part of the network is STRIVE-1, exploring whether the antiviral medication ensitrelvir can reduce symptoms and duration of hospitalization in persons with moderate to severe COVID-19. Another STRIVE COVID-19 study is exploring the additional use of immunomodulating agents for hospitalized patients.
Beyond COVID-19, we completed enrollment for a few other studies, including an mRNA shingles vaccine study by Pfizer and an exciting novel dual-affinity retargeting molecule for HIV. There are other studies we anticipate opening in 2025, including a C. difficile vaccine, as well as several HIV prevention and treatment studies.
Dr. Liu: We will never forget how the COVID-19 pandemic changed our lives. Thanks to tested vaccines and treatments, we are able to return to a normal life of packed movie theaters and lecture halls. Some of our team of skilled and knowledgeable research staff are being transferred to other areas where groundbreaking research is occurring throughout the Mount Sinai Health System. We are forever grateful for the contributions of the COVID CTU in reducing the morbidity and mortality from the COVID-19 pandemic.