A Mount Sinai Medical Student, Whose Work Helped a Young Boy Recover From Nearly Drowning, Reflects on Her Research and Aspirations

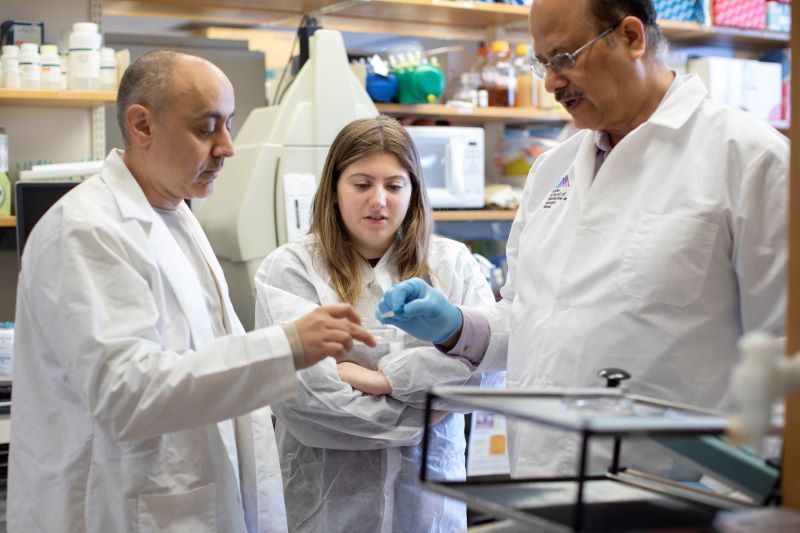
From left: Farid Khan, MBBS, co-chair of the Fellows in Training Program of the New York Chapter of the American College of Cardiology; Helen Gordan; and Samuel Kim, MD, the chapter’s program chair
Helen Gordan, a second-year medical student at the Icahn School of Medicine at Mount Sinai, recently won best clinical case abstract at the New York Chapter of the American College of Cardiology Fellows in Training competition.
Her abstract titled “Unraveling a Genetic Diagnosis After a Near Drowning Incident” describes the diagnostic odyssey of a 9-year-old boy who was cared for at Mount Sinai Kravis Children’s Hospital after he was resuscitated from near-drowning in a swimming pool.
Careful sleuthing ultimately elicited a novel cardiac genetic cause. The patient made a full recovery and is being treated successfully, and the genetic discovery will permit others to benefit in the future.
Ms. Gordan’s award is all the more impressive for having won it as a second-year medical student, competing against much more senior trainees in internal medicine and cardiology fellowship training. Ms. Gordan presented the work in an oral presentation in December.
In a Q&A, Ms Gordan discusses why she chose the Icahn School of Medicine at Mount Sinai, what has drawn her to explore pediatric cardiology as a potential career choice, and her research interests.
What inspired you to explore pediatric cardiology as a medical student?
From the beginning of medical school, I was drawn to specialties that offer meaningful long-term patient relationships and combine medical management with precise interventions. Pediatric cardiology fulfills both these criteria and more. Since every heart is unique, cardiologists must rely on fundamental physiologic principles to tailor treatments to each case. The opportunity for early intervention, especially in congenital heart defects, has an immeasurable impact on long-term outcomes, enabling children to thrive and lead full lives. It opens the door to the kind of long-term relationships with patients and families that I desire in my career.
What are your research interests?
My research interests lie at the intersection of engineering and clinical care. My undergraduate degree is in electrical engineering, so I am particularly interested in how technology can be harnessed to both enhance therapeutic outcomes and improve access to care for underserved populations. For example, asynchronous online care platforms—which allow physicians to assess patient concerns and provide treatment through messaging, patient portals, or online questionnaires— offer unique opportunities to bridge gaps in accessibility, especially for resource-limited settings. Understanding how these models can integrate with chronic disease management, including heart disease, is a growing area of interest.
What does winning this abstract award mean to you and how will it help propel your studies?
I was incredibly excited and honored to win this case competition. It has encouraged me to continue to explore challenging questions and raise questions about frameworks for diagnoses. It has allowed me to receive feedback from experts that have both refined my skills and broadened my perspective. Most importantly, it has underscored the importance of great mentorship and collaboration. I am incredibly grateful for the support I received from Dr. Barry Love and Dr. Amy Kontorovich while working on this case.
Why did you choose the Icahn School of Medicine school and how has the medical school experience been so far?
The Icahn School of Medicine stood out to me because of its emphasis on fostering diverse academic backgrounds. Coming from an engineering discipline, I was eager to join a medical institution that values multidisciplinary approaches to problem-solving and allows students to incorporate their own interests into their clinical training. The culture of innovation and research has completely exceeded these expectations. I have been able to learn about entrepreneurship in medicine through Sinai BioDesign’s THRIVE program, explore access-to-care barriers through a summer global health research program, and explore different specialties with the support of amazing faculty. My experience has been exceptional, largely due to the supportive mentorship I’ve received from Dr. Love, Dr. Gault, and many others.
What do you hope your impact will be on patients, field, and practice?
First and foremost, I hope to be an exceptional clinician. I would like to provide the expertise and empathy patients need when facing scary and vulnerable moments. I also aspire to combine innovation with equitable care to make an impact. I hope to provide solutions that enhance quality of life while ensuring accessibility to care, regardless of socioeconomic or geographic barriers. Ultimately, I want my career to serve as a bridge between disciplines and help to drive advancements that improve both individual patient experiences and systemic health care delivery.